Hard-to-treat cancers
Overview
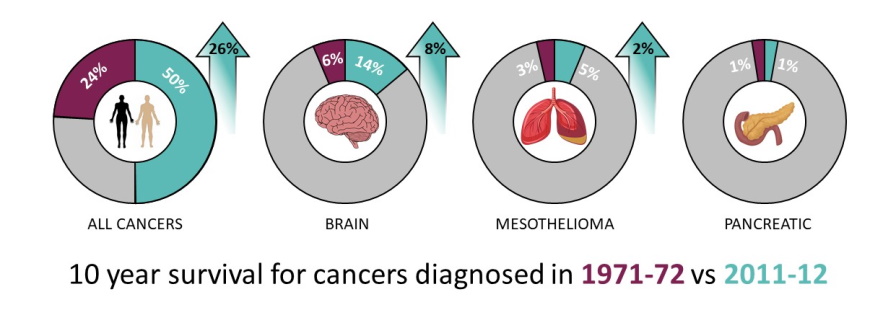
The cancers in the sights of the IRC – glioblastoma, mesothelioma and pancreatic cancer – are hard-to-treat because they come with their own defence mechanisms. Brain tumours such as glioblastoma have ill-defined boundaries, making them difficult to fully remove surgically, while also being protected from conventional chemotherapy drugs by the blood-brain barrier. Pancreatic and mesothelioma tumours have fibrous outer layers making drug penetration problematic.
The overarching engineering challenge associated with hard-to-treat cancers is to increase cell-destroying drug concentration within the tumour itself while avoiding toxicity elsewhere. Two issues arise: (i) traditional targeted drug delivery strategies suffer from limited capacity of the delivery vehicles preventing sufficient drugs reaching the cancer site which restricts the efficacy of treatment; and (ii) to access the tumour the drug needs to cross endogenous barriers – natural defence mechanisms – which include the blood brain barrier (BBB) and tissue stroma.
Ideally, to better combat hard-to-treat cancers, new technologies will target multiple therapeutic pathways including immune/inflammatory; neoangiogenic, and cell proliferative. Taking a multimodal delivery approach will converge on the tumour to deliver high levels of drugs to the targeted cells for maximum therapeutic effect.
